Patient Resources
We hear a great deal about prevention and early detection in cancer. While cancer prevention may never be 100 percent effective, many things (such as quitting smoking and eating healthy foods) can greatly reduce a person’s risk for developing cancer, the causes for IBC are unknown and there is not a form of detection prior to a stage three.
This lack of early detection can cause great emotional stress, so it is important that if you are diagnosed with IBC to understand your late stage diagnosis was not your fault. There is not a way to know you have IBC until the outward physical signs are presented.
We would like to give a very brief overview of some common challenges to diagnosis.
Why are mammograms notoriously ineffective in detecting IBC?
IBC doesn’t form a discrete lump that can be seen easily and measured. However, IBC does have other features that can be observed on a mammogram if the radiologists are trained on what to look for. These signals of IBC include trabecular distortion, skin thickening and retraction of the skin and nipple. Another reason is that in younger women especially who have denser breasts, mammograms lose sensitivity because more of the breast is white on a mammogram.
Can IBC be confirmed on a biopsy alone?
The biopsy may not find cancer due to the nature of the disease, so more than one biopsy maybe required or further testing such as a MRI. Also if the patient does not have a palpable lump, (only a faction do present with a lump) cord needle might not be possible, so a skin punch biopsy of red or suspicious area could be the next step in obtaining a diagnosis.
A note about treatment from Terry Arnold, Founder of the IBC Network Foundation:
“I would like to offer my thoughts on treatment of inflammatory breast cancer based on my experience and education of the disease. I see many women having chemotherapy followed by a mastectomy with same-day reconstruction, which delays radiation and could allow time for the cancer to grow. Remember, there is a reason for that radiation; it is a very important part of the IBC care protocol. Women often tell me there was no discussion with their cancer team that it might be best to wait for reconstruction, or even if having reconstruction is a healthy option for them.
I am not laying this message out here to get anyone all up in arms that their caregiver is not a good one. I am happy for those sisters who have reconstruction, as long as it is later and not at the risk of their care. In a world of “we are not defined by our cancer” or “my cancer was just a bump in the road” banter, the message for a cancer patient to delay or Heaven forbid, not have reconstruction at all is a hard one to get out. The message is an important one because IBC is a different type of breast cancer and has a different standard of treatment that is based upon how IBC grows and spreads in the body. If your treatment for IBC was not in the order listed or if you had reconstruction while still in treatment, again, that does not mean you are doomed. IBC is a very sneaky disease, and to be best able to beat our cancer we have to understand our cancer.”
– Terry Arnold
The standard of treatment for this disease is:
– Chemotherapy
– Surgery, which is a mastectomy, a radical one, which is not skin sparing. (Some doctors are suggested not removing the breast, very case by case issue.)
– Pathology, if it comes back clear, you move to radiation. If pathology is not clear, possible to have more chemotherapy but more likely to be moved into radiation.
– Six weeks of daily radiation, sometimes twice a day depending on the needs of that patient.
– Then if possible, reconstruction after a waiting period of maybe as much has two years for many reasons….hopefully not one with metal implants that will limit future testing. Shocking to hear, but I have met women who had to have their post cancer implants removed to allow for testing!
Treatment centers
Inflammatory breast cancer (IBC) is a unique form of breast cancer, marked with rapid onset and also physical changes that can often be mistaken for an infection or an injury. In a matter of days or a few weeks, the breast can appear swollen due to cancer cells blocking lymph vessels in the skin, and this can cause redness of the breast skin, nipple distortion and pain. IBC typically does not present with a lump, making IBC more difficult to detect using standard screening technologies.
Just like IBC presents differently and has different diagnosis needs, the standard of care is different from general forms of breast cancer. Due to the rarity of the disease, IBC diagnosis and treatment is not commonly taught in medical or nursing schools. Patients can be very discouraged to meet with their local medical team to find out that if their oncologist, has treated an IBC patient in the past, it might have been only a few of them in a full career in medicine, if any at all.
There are a few phrases heard in the IBC world but rarely do you see a definition associated with the phrase: “multidisciplinary clinic” and “trimodal care” for example. These phrases are a direct reflection of the unique needs in care for this complex disease – tackling both local disease in the breast and distant disease possibly circulating in the blood early after diagnosis.
What is trimodal care?
Trimodal care would include systemic therapy (chemotherapy and targeted therapies) given by medical oncologists, breast cancer surgeons, and radiation oncologists who have specific expertise in treating IBC. This unique team needs to work together, and closely monitor the patient due to the aggressive nature of this type of breast cancer. The goal of chemotherapy as a first step is to render the patient a surgical candidate, however the timing of surgery must be coordinated so it is done at the correct time. In IBC it is especially crucial that the tri-modal team ensures that the patient is responding well before surgery but are mindful not to miss the surgical window since even local control can be a quality of life factor to strongly consider. The steps of trimodal treatment for IBC are in the schematic linked here.
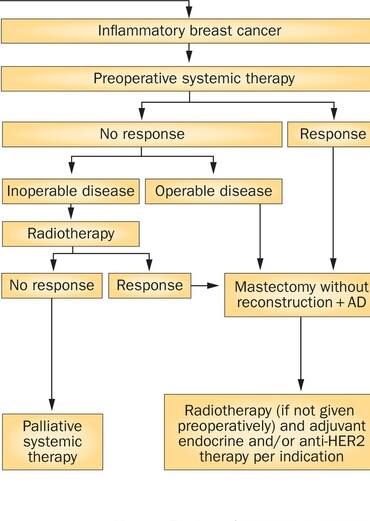{kind=link}
What should a trimodal clinic (multidisciplinary clinic) consist of?
A multi-disciplinary clinic for IBC would include medical oncologists, breast cancer surgeons, and radiation oncologists who have specific expertise in treating IBC. Such clinics are not common and the few that are operating in the US are based out of university centers. These university-based hospitals are also conducting and publishing IBC research and creating IBC focused clinical trials based off this research and through building relationships with drug companies. These programs include research scientists, pathologists, radiologists, medical oncologists, surgeons, radiation oncologists, plastic surgeons and lymphedema specialists. All the medical teams working together assure that the IBC patient doesn’t fall thru the cracks and receive the proper care required for this aggressive disease and to help them live as full lives as possible after their treatment is complete.>


We would be remiss not to mention Dr. Massimo Cristofanilli, MD who is viewed as one of the world’s leading experts on IBC. He is a medical oncologist with many years of experience in treating aggressive cancers including IBC and is internationally known in breast cancer drug development. He practices at Northwestern University in Chicago, Illinois where he leads a center for molecular medicine and performs research into the use of liquid biopsies in IBC.
As interest is growing in IBC care, some positive changes are coming. Clearly to have IBC research done at all/most hospitals or cancer centers is cost prohibitive based on the incidence of this cancer. In addition, research resources are limited however, there are medical centers that wish to be known as Centers of Excellence for IBC. These centers will have teams especially trained to give the proper standard of care for IBC without the research component. As these centers are developed, we will add them to this article.
We do not wish to cause concern if you are not able to receive your treatment at a specialty center. We have seen excellent care by community doctors, but this is not the norm, especially when the cancer does not respond well to initial chemotherapy. However we wanted to address this topic as it is a common question. As IBC awareness and education is growing, we hope to see more options for patients regardless of location.
Have insurance questions? See this link.