guest post by Dr Angela Alexander, a TRIUMPH translational postdoctoral fellow at MD Anderson. Her laboratory work focuses on combinatorial treatment approaches to benefit IBC and TNBC patients. Her full bio is at the end of this post and we are so grateful for her generous of time and experience to share this information with our reader.
Thank you Dr. Alexander!
As a breast cancer researcher in a mainly TNBC-lab, I get asked sometimes about the latest in research regarding TNBC and what sorts of options are available for patients. In this post I thought I would go over what sorts of trials are available and accruing right now at MD Anderson and several other large centers across the country and what science they are based on.
First though, one of the most interesting recent laboratory advances came out of Jennifer Pietenpol’s lab at Vanderbilt, where Lehmann and colleagues performed gene expression analysis on a large number of TNBC tumors and identified 7 different subtypes of TNBC each with some potential targets and deregulated pathways predicting sensitivity to different drugs. There are 2 subtypes that are basal like, 2 mesenchymal subtypes, a luminal subtype that expresses the Androgen Receptor as well as an immunomodulatory subtype. To read the paper where these subtypes were described, see (1).
More recently, Naoto Ueno’s lab asked whether these subtypes have prognostic value i.e. if we could identify upfront which subtype an individual patient’s tumor most resembles, can we determine their likely clinical response to neoadjuvant chemotherapy. Of course I wouldn’t be writing about this if the answer wasn’t yes, and these results were quite intriguing (2). Moving forward however, in order to translate these findings into routine practice a number of steps will be required, including prospectively validating the Ueno study, determining whether overall survival rates are also predicted by subtype, then hopefully going through the CLIA-certification process to convert the currently research-based microarray method into a robust analysis approach on live patient samples. Stay tuned for more on these subtypes over the coming years!
Back to the major theme of the post however – what options are available today for TNBC patients. Read on for what are the most promising angles of clinical and translational research or visit the tl;dr version of this info (a table with drugs and links)
PARP inhibitors – alone and in combination
First up: PARP inhibitors – one of the hottest areas of research in TNBC. PARP inhibitors are drugs that inhibit repair of DNA damage (one of the ways that chemotherapy kills cancer cells). Initially when studied in unselected populations, the response rates were not that high…but as the preclinical work has demonstrated increased sensitivity in BRCA1/2 mutant cell lines/tumors and more selected trials done, the results have been more promising. Since about 70% of BRCA1/2 mutant breast cancers are triple negative, many of these studies use TNBC status, as well as young age, as a reasonable rationale to screen for mutations which would allow trial participation.
There are quite a few of these drugs in trials, and so far we have learned that they have a great safety profile. In the following sections with links to trials, I will use the following abbreviations for sites that come up multiple times: MDA = MD Anderson, MSKCC = Memorial-Sloan Kettering, DFCI = Dana Farber Cancer Center, FHCC = University of Washington Fred Hutchinson Cancer Center, NIH = National Institutes of Health.
Regarding PARP inhibitors, there are at least 2 phase 1 trials of newer PARP inhibitors as single agents to examine safety and hopefully gain early hints of efficacy.
Single agent trials:
1) BMN 673, in solid tumors including breast cancer – http://clinicaltrials.gov/ct2/show/NCT01286987 (Open: MDA, TGen, UCLA, others….)
2) Rucaparib – http://www.clinicaltrials.gov/ct2/show/NCT01482715 (Open: DFCI)
Moving forward however, it is more likely that PARP inhibitors will need to be used in combination with other drugs to have meaningful activity. These studies will be based on pre-clinical evidence of synergy, such as using PARP inhibitors to potentiate DNA damage by cytotoxic chemotherapy or other targeted agents that work via similar pathways. On my blog, last year I wrote about 2 very nice Cancer Discovery papers that designed one such combination – ie PI3K inhibitors with PARP inhibitors (3+4). To read more, you can visit that post.
Combination PARP inhibitor trials:
1) Here is the trial with Olaparib (PARP inhibitor) and BKM120 (PI3K inhibitor) – http://clinicaltrials.gov/ct2/show/NCT01623349 (Open: MDA, MSKCC, DFCI, others)
2) Another quite reasonable combination is a Veliparib/ABT-888 (PARP inhibitor) with carboplantin – http://clinicaltrials.gov/ct2/show/NCT01149083 (Open: 21 sites including MDA, MSKCC, DFCI…)
3) Other chemotherapy combinations include this study with Veliparib in combination with either temozolomide or carboplatin & paclitaxel – http://www.clinicaltrials.gov/ct2/show/NCT01506609 (Open: MDA, DCFI and 90 other centers worldwide!) or Veliparib + cisplatin + vinorelbine – http://www.clinicaltrials.gov/ct2/show/NCT01104259 (Open: FHCC)
4) In a setting of a loco-regional recurrence of TNBC or IBC in a location that is amenable to radiation (ie no previous chest wall coverage), there is also a trial available using Veliparib as a radiosensitizer. Trial info –http://www.clinicaltrials.gov/ct2/show/NCT01477489 (Open: MDA, MSKCC, DFCI, Duke, Uni of Michigan)
The majority of the above trials (other than the radiation one) use BRCA1/2 mutation status as an inclusion criteria. So if the PARP inhibitor studies are not options based on being BRCA1/2 wild-type (ie negative for any known mutations), there are a good number of other options as outlined in the next sections.
Cell cycle checkpoints
One of the other new therapeutic vulnerabilities in TNBC is deregulated cell cycle checkpoints. A couple of options currently exist based on preclinical data. The lab that I am pursuing my postdoctoral work has been working on one of these for several years. We have found that the majority of TNBCs have a protein called cyclin E that is cleaved and mislocalized in the cytoplasm causing it to be oncogenic due to high activity of its binding protein CDK2, and that cell lines with high levels of cyclin E in the cytoplasm are exquisitely sensitive to drugs that inhibit CDK2 (5). Specifically the trial we have open right now is a combination of the CDK inhibitor (Dinaciclib) with epirubicin. The trial info is here – http://clinicaltrials.gov/ct2/show/NCT01624441 (Open: MDA).
You might’ve heard of the p53 gene, which is one of the most commonly mutated tumor suppressor genes in cancer, including TNBC. One of the consequences of p53 mutation is loss of cell cycle checkpoints that normally protect cells from too much DNA damage. In the past few years it has become clear that p53 mutant cells are sensitive to inhibitors of another cell cycle checkpoint protein called Wee1 (6). In addition Wee1 inhibitors synergize with chemotherapy in cells (7). AstraZeneca recently licensed Merck’s Wee1 inhibitor called MK-1775 that works well in cell lines, and now is being studied in several phase 1 trials. TNBC patients might be eligible for this study of MK-1775 http://clinicaltrials.gov/ct2/show/NCT01748825 (Open: NIH).
Targeting Growth Factor Signaling Pathways
a) PI3K-AKT-mTOR pathway:
Another potential targeted therapy option is targeting the PI3K/AKT pathway, since this pathway is frequently altered in breast cancer, and multiple growth factor survival signaling pathways converge on AKT and mTOR (see figure 1 for a simplified schematic of the proteins in the pathway and how they can be targeted). In addition, there is a recent study that shows that in residual tumors in TNBC patients after standard anthracycline-taxane chemotherapy, several PI3K pathway proteins are activated and correlate with relapse-free survival, suggesting again this pathway is relevant therapeutically (8). However it is currently not known where along the pathway would be best to target, so there are drugs that target many components of the pathway and even dual kinase inhibitors such as GDC-0980. There are a few biomarkers of pathway alterations that appear to predict response to this class of agents, so some of these trials select only these patients.
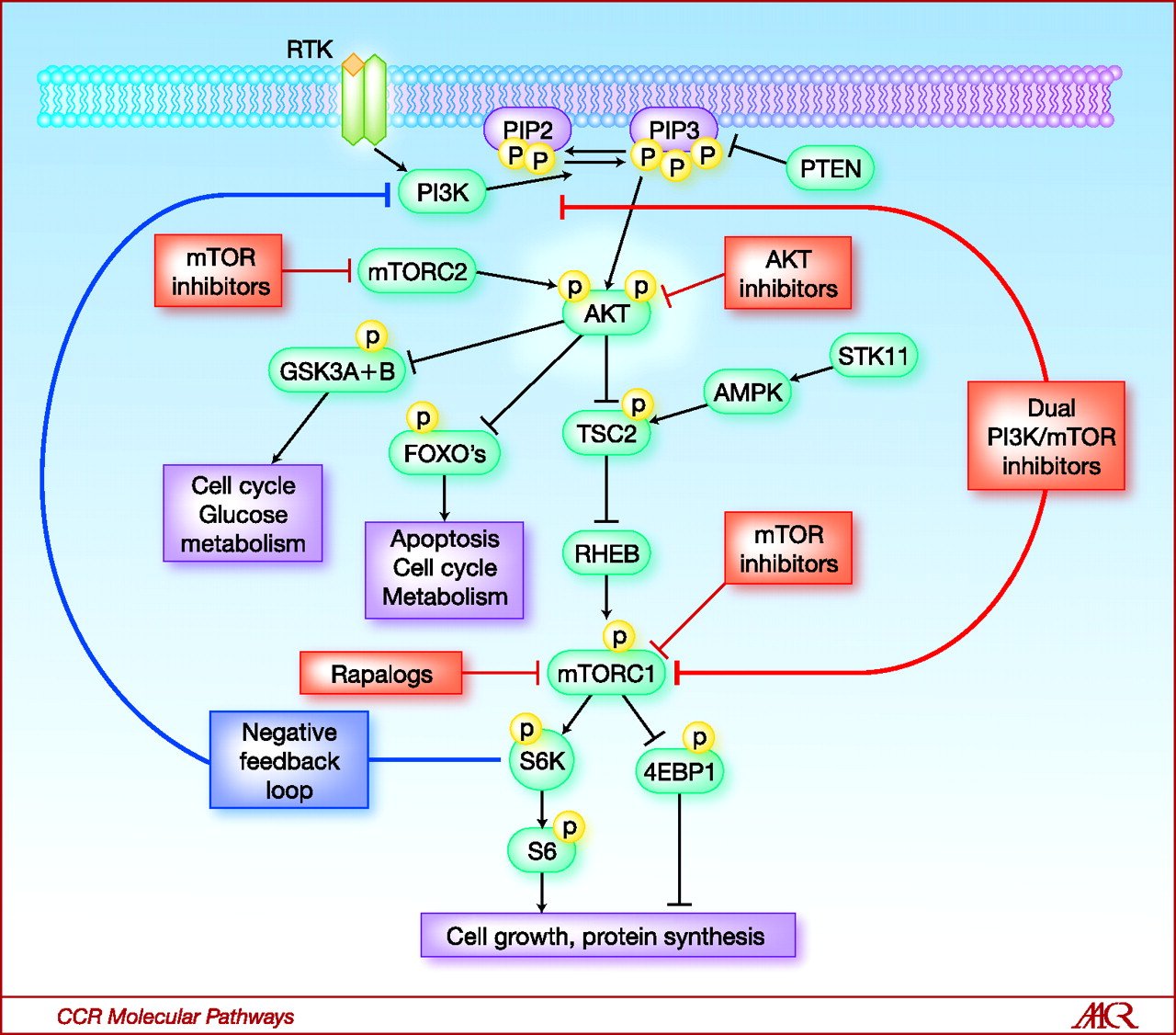
Figure 1: PI3K pathway schematic showing proteins and potential targeting mechanisms
One trial is a phase 2 trial of Merck’s AKT inhibitor (MK-2206) for advanced breast cancer patients with PIK3CA or AKT mutation or PTEN alterations. The trial info is – http://www.clinicaltrials.gov/ct2/show/NCT01277757 (Open: MDA, DFCI, Vanderbilt, and 2 other centers).
Drugs that target PI3K (upstream of AKT) are further along in development and there are more of them. Two PI3K inhibitor trials that are open to TNBC patients are:
1) BKM120 – http://www.clinicaltrials.gov/ct2/show/NCT01790932 (Open: DFCI)
2) GDC-0941 in combination with paclitaxel, with or without bevacizumab (an angiogenesis inhibitor) –http://www.clinicaltrials.gov/ct2/show/NCT00960960 (Open: DFCI)
b) Growth factor receptors: cMet and EGFR
The other new signaling target that is promising is cMet which is a growth factor receptor that is found to be overexpressed in 60% of TNBCs and highly active in about 35% (9). There are a number of drugs being tested that target cMet including antibodies and small molecule inhibitors. In the interest of full-disclosure of an incidental discovery while searching for something else recently, I discovered that Roche have discontinued development of the cMet-targeting monoclonal antibody (MetMab) in the TNBC setting. Given no other specific news, one could speculate that the response rate was pretty low.
1) One open study is of a dual cMet-ALK inhibitor X-396, which you can read more about here – http://clinicaltrials.gov/ct2/show/NCT01625234 (Open: MDA, Vanderbilt and Sarah Cannon Research Institute)
2) Another oral cMet-inhibitor being studied is ARQ197. The trial specifically for metastatic TNBC patients is here – http://www.clinicaltrials.gov/ct2/show/NCT01542996 (Open: DFCI and Brigham and Women’s Hospital)
3) A third cMet inhibitor XL184 trial is even more interesting, since this molecule also inhibits VEGFR2 which plays a role in angiogenesis, and is found to be amplified in about a third of TNBCs and linked to poor prognosis. Therefore this trial has potential to inhibit 2 important processes for TNBC cell survival. Trial info – http://www.clinicaltrials.gov/ct2/show/NCT01738438 (Open: DFCI and related centers in Boston)
Targeting EGFR has been attempted for a while, but the jury is still out whether this target is going to pan out. EGFR is known to be overexpressed in a large fraction of TNBCs, and the preclinical work has been quite exciting with regard to the ability to block cell migration and metastasis in mouse models, as well as block repair of DNA damage, leading to cell death. However, moving these studies into the clinic has been somewhat challenging for a number of reasons. One is that the EGFR antibodies are quite toxic. Secondly, although there are a few signals of (short-term) response, we have certainly not identified the specific patient population who does benefit from these agents. This year a phase 2 study of the EGFR antibody Cetuxumab in combination with cisplatin in unselected metastatic TNBC patients was published by Jose Baselga and colleagues, which showed a doubling in objective response rate (from 10-20%) – but this was not a large enough difference to meet the trial’s pre-defined criteria (10).
An alternative approach to target this important pathway is via oral tyrosine kinase inhibitors which may have different activities and toxicities from the antibodies such as Cetuximab. To understand these further, a trial with Erlotinib is available, examining its use in a maintenance setting after treatment with nanoparticle-encapsulated Paclitaxel (known as Abraxane) and Bevacizumab (the anti-angiogenesis drug mentioned previously). An interesting concept. see here for details – http://www.clinicaltrials.gov/ct2/show/NCT00733408 (Open: FHCC and 15 other centers)
c) Miscellaneous other signaling inhibitors
Inflammation from the tumor microenvironment has been linked to tumor growth due to stromal and immune cells secreting factors that signal through cytokine receptors. One example of such a pathway that has been found to be important and potentially targetable is the interleukin and JAK-STAT pathway. A few years ago, a nice paper came out showing that the IL6-JAK2-STAT3 pathway is enriched in stem-like cells in breast cancer (11). Following up on this observation, at the recent ASCO Breast Cancer Symposium, Beth Overmoyer’s group also presented correlative data showing concomitant activation of the JAK2 and mTOR signaling pathways in IBC patient samples’. This suggest that in the future a combination of JAK2 inhibitor with an mTOR inhibitor might be examined. Based on this preclinical data showing the importance of this pathway, a JAK2 inhibitor, Ruxolitinib is being investigated in a combination TNBC and IBC (any receptor status) trial. Eligible patients must undergo a research biopsy to test for a biomarker in the JAK-STAT3 pathway i.e. phosphorylated Stat3, which is seen in ~60% of IBC patients. The trial info is here – http://www.clinicaltrials.gov/ct2/show/NCT01562873 (Open: DFCI and soon other center(s)).
Another growth pathway that has been associated with a large portion of TNBCs involves the protein Src, which is a protein that signals upstream of various pathways that control proliferation, migration, differentiation, angiogenesis etc (12). Consequently inhibitors of Src have been considered. Clinically though, even the potent Src inhibitor Dasatinib as a single agent has not shown much activity in unselected patients (13), but since the preclinical work indicated synergy with standard chemotherapies such as taxanes, it is now being tested in combination with weekly paclitaxel in this broad MBC trial – http://clinicaltrials.gov/ct2/show/NCT00820170 (Open: MSKCC)
d) Angiogenesis targeting
Angiogenesis inhibitors have been studied for several years now based on solid rationale, but their optimal role in breast cancer treatment is still unknown. Bevacizumab (Avastin) is probably the best studied drug that has shown similar statistically significant benefit in TNBC patients as other subtypes when combined with chemotherapy in the first-line metastatic setting. However the very large 2600-patient BEATRICE study which was performed in the adjuvant setting with chemotherapy demonstrated that TNBC patients did not derive any additional benefit from Bevacizumab than chemotherapy alone in reducing recurrence.
This cautioned enthusiasm for VEGF targeting (in selected patients) has led to development of further agents that also target angiogenesis. One such agent is the VEGF receptor inhibitor Tivozanib, which has been developed furthest in RCC. It is now being studied in TNBC in a placebo-controlled combination study with paclitaxel – see http://www.clinicaltrials.gov/ct2/show/NCT01745367 (Open: DFCI and up to 46 other centers eventually, see list on the trial link)
Immunotherapy
Probably the newest area of interest in TNBC biology is harnessing the potential of the immune system in iradicating tumors. Many cancers including TNBC actively evade detection and eradication by the immune system via expressing proteins such as PD-L1 and PD-L2 on their cell surface. These proteins interact with receptions found on T-cells called PD-1 which blocks the T-cell mediated anti-tumor killing ability. In fact, the data presented at ASCO earlier this year in melanoma and lung cancer using antibodies that block this interaction, were so promising that some oncology thought leaders are already calling these the Drug of the Year.
With respect to TNBC now, there is a phase 1b trial that is currently open using Merck’s PD-1 inhibitor Lambrolizumab (MK-3475) that includes 3 patient cohorts, one of which is TNBC. The inclusion criteria are quite broad, so check it out – http://www.clinicaltrials.gov/ct2/show/NCT01848834 (Open: FHCC, Moffitt Cancer Center and other mystery sites in IL, MA, NC, PA, WA)
Another variation on immunotherapy is targeting a specific type of myeloid immune cell called macrophages. Elevated numbers of macrophages have been found in residual tumors from patients who did not achieve a pCR with neoadjuvant chemotherapy (14). Why is this? Could be for a number of reasons – including macrophage suppression of T-cells and cytokine secretion that promotes angiogenesis. Therefore targeting these cells has been proposed as a way to boost natural immunosurveillance. There are 2 trials open now testing combinations of chemotherapy with immunotherapy:
1) Eribulin (a microtubule-targeting chemotherapy) with the ‘macrophage inhibitor’ PLX3397 (CSF-1 inhibitor) is currently underway in an all-comers metastatic breast cancer trial, see http://clinicaltrials.gov/show/NCT01596751 (Open: UCSF, future at Duke and VICC)
2) An even broader study for solid tumors including TNBC of PLX3397 with weekly paclitaxel is also available – http://www.clinicaltrials.gov/ct2/show/NCT01525602 (Open: UCSF, Ohio State)
Finally another metabolic mechanism of immunosuppression, via the IDO pathway is being targeted in metastatic breast cancer in combination with docetaxel. The IDO inhibitor being studied is Indoximod (1-methyl-D-tryptophan) http://clinicaltrials.gov/show/NCT01191216 (Open: Moffitt, Emory, and several other centers)
References:
(PDFs available upon request by email)
(1) Lehmann B, et al, “Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies” JCI 2011 (http://www.ncbi.nlm.nih.gov/pubmed/21633166)
(2) Masuda H et al, “Differential response to neoadjuvant chemotherapy among 7 triple-negative breast cancer molecular subtypes”, Clin Cancer Res 2013 (http://www.ncbi.nlm.nih.gov/pubmed/23948975)
(3) Ibrahim YH et al, “PI3K inhibition impairs BRCA1/2 expression and sensitizes BRCA-proficient triple-negative breast cancer to PARP inhibition”, Cancer Discovery 2012 (http://www.ncbi.nlm.nih.gov/pubmed/22915752)
(4) Juvekar A et al, “Combining a PI3K with a PARP inhibitor provides an effective therapy for BRCA1-related breast cancer”, Cancer Discovery 2012 (http://www.ncbi.nlm.nih.gov/pubmed/22915751)
(5) Nanos-Webb A et al, “Targeting low-molecular weight cyclin E (LMW-E) in breast cancer”, Breast Cancer Res Treatment 2012, (http://www.ncbi.nlm.nih.gov/pubmed/21695458)
(6) Aarts M et al, “Forced mitotic entry of S-phase cells as a therapeutic strategy induced by inhibition of WEE1”, Cancer Discovery 2012 (http://www.ncbi.nlm.nih.gov/pubmed/22628408)
(7) Hirai H et al, “Small-molecule inhibition of Wee1 kinase by MK-1775 selectively sensitizes p53-deficient tumor cells to DNA damaging agents” Mol Cancer Ther 2009 (http://www.ncbi.nlm.nih.gov/pubmed/19887545)
(8) Sohn J et al, “Functional proteomics characterization of residual triple-negative breast cancer after standard neoadjuvant chemotherapy”, Ann Oncol 2013 (http://www.ncbi.nlm.nih.gov/pubmed/23925999)
(9) Raghav, KPS et al, “cMet and phosphor-cMET protein levels in breast cancers and survival outcomes”, Clin Can Res 2012 (http://www.ncbi.nlm.nih.gov/pubmed/22374333)
(10) Baselga, J et al, “Randomized phase II study of the anti-epidermal growth factor receptor monoclonal antibody Cetuximab with cisplatin versus cisplatin alone in patients with metastatic triple-negative breast cancer”, J Clin Oncol 2013 (http://www.ncbi.nlm.nih.gov/pubmed/23733761)
(11) Marotta LL et al, “The JAK2/STAT3 signaling pathway is required for growth of CD44+/CD24- stem-like breast cancer cells in human tumors”, JCI 2011 (http://www.ncbi.nlm.nih.gov/pubmed/21633165)
(12) Tryfonopoulos D et al, “Src: a potential target for the treatment of triple-negative breast cancer” Ann Oncol 2011, (http://www.ncbi.nlm.nih.gov/pubmed/21357651)
(13) Finn RS et al, “Dasatinib as a single agent in triple-negative breast cancer: results of an open-label phase 2 study”, Clin Cancer Res 2011 (http://www.ncbi.nlm.nih.gov/pubmed/22028489)
(14) Ruffell B et al, “Leukocyte composition of human breast cancer” PNAS 2011 (http://www.ncbi.nlm.nih.gov/pubmed/21825174)
tl;dr version
Graphic permission:
Figure 1: PI3K pathway schematic showing proteins and potential targeting mechanisms
About Dr. Alexander
Dr Angela Alexander is a TRIUMPH translational postdoctoral fellow at MD Anderson. Her laboratory work focuses on combinatorial treatment approaches to benefit IBC and TNBC patients. Prior to this, she obtained at her PhD also at MD Anderson in the Department of Molecular Carcinogenesis working on response mechanisms to cellular damage and stresses. Currently in her spare time outside of work, she volunteers for The IBC Network, writes a blog at http://thecancergeek.wordpress.com, and enjoys talking to patients and other scientists on social media. She can be contacted at th***********@***il.com or on twitter (@thecancergeek) with any questions or comments on her posts.